


De-icing the Mystery Behind Hemiplegic Frozen Shoulder
If you have attended a Saebo course in the past, you most likely have heard the comment “it is the hand that guides the arm”. Although this is theoretically true when discussing the importance of incorporating one’s hand functionally, broadly speaking however, we should avoid providing too much importance to the hand as it is only one element of the interdependent kinetic chain. Yes, the hand mainly guides the arm to interact and problem-solve the environment, however, if pain and limited motion exists proximally (i.e., shoulder), function will be compromised regardless of the hand’s ability to participate.
One of the main goals of the shoulder and elbow is to position the hand for function. To maximize clinical outcomes for our hemiparetic clients, we must not only incorporate evidenced-based principles to improve arm and hand function, but we should also remain committed to preventing or reversing shoulder pain and stiffness. Upper limb pain and loss of motion continues to be problematic for clinicians and patients. One of the main clinical conditions associated with pain and stiffness is Frozen Shoulder. The purpose of today’s post is to discuss the key facts and possible causes of this debilitating condition. In addition, I will also briefly touch on the pathomechanics, as it relates to Frozen Shoulder, for both the flaccid and spastic stages of motor recovery.
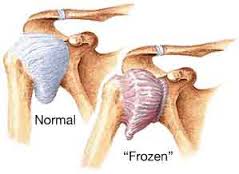
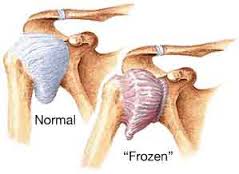
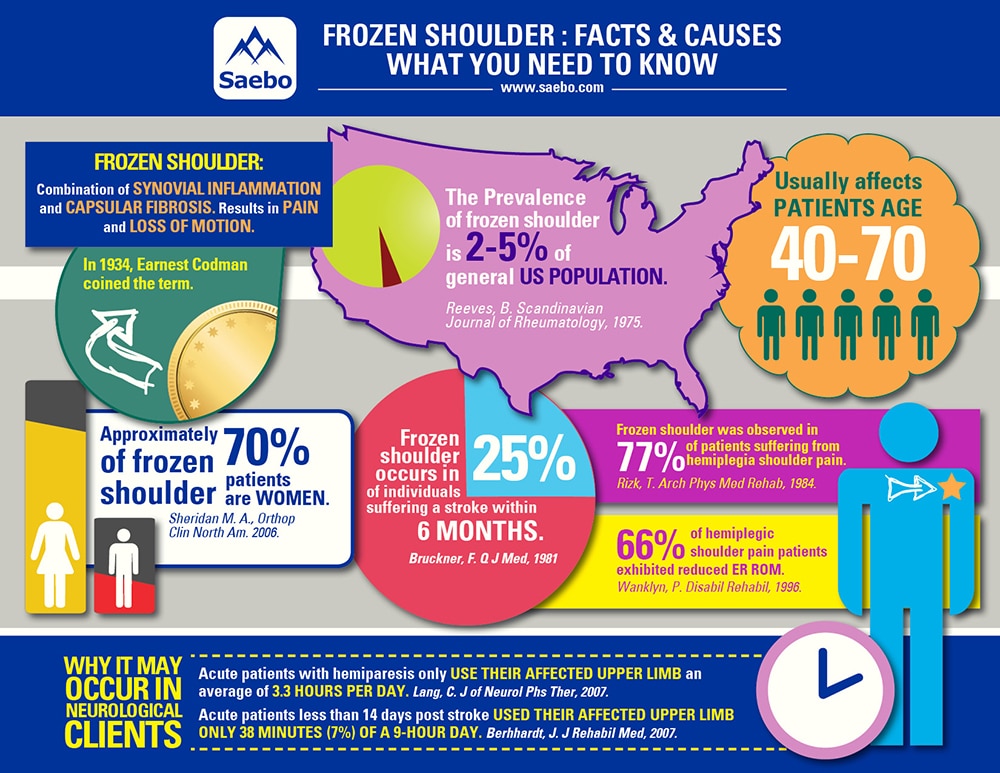
Frozen Shoulder, also known as adhesive capsulitis, immobilization arthritis, stiff shoulder or capsular pattern, is a common condition involving shoulder pain and loss of motion. It is thought to be a combination of synovial inflammation and capsular fibrosis. The term “Frozen Shoulder” was first coined by Earnest Codman (Boston Surgeon) in 1934 and refers to shortening of the glenohumeral joint capsule and ligaments. He expressed that the condition is “difficult to define, difficult to treat, and difficult to explain” from a pathological standpoint. In 1945, Nevasier was the first to identify the pathology through histological and surgical examination. He concluded that Frozen Shoulder is a thickening and contracture of the capsule which becomes adherent to the humeral head. He later termed the condition “Adhesive Capsulitis”. Nevasier described it as an inflammatory reaction that caused the adhesions to the joint capsule.
The current definition of Frozen Shoulder by the American Shoulder and Elbow Surgeons is “a condition of uncertain etiology characterized by significant restriction of both active and passive shoulder motion that occurs in the absence of a known intrinsic shoulder disorder”. Neviaser et al. described Frozen Shoulder as a “waste-can diagnosis” because it was over-used and inappropriately applied to patients with other painful shoulder conditions that led to stiffness. For example, there are numerous clinical conditions and pathologies (arthritis, rotator cuff tears, trigger points, spasticity) that can cause pain and stiffness, but are in absence of capsular contracture and restriction in passive range of motion typical of a Frozen Shoulder. The clinical history and physical exam will be paramount in differentiating between the stiff and painful shoulder and a true Frozen Shoulder.
In addition to being a common orthopedic condition, this painful and debilitating disease affects a large percentage of neurologically impaired clients as well. Several studies suggest that Frozen Shoulder may be one of the most significant causes of shoulder pain after stroke. It can occur in up to 25% of individuals suffering a stroke within 6 months. In addition, Frozen Shoulder can also be observed in up to 77% of patients suffering from hemiplegic shoulder pain.
Because confusion sill exists over the etiology and pathophysiology of the disease, it continues to be challenging to pinpoint whether the client is suffering from a painful and stiff shoulder or a true Frozen Shoulder (capsular adhesions and synovial inflammation). Regardless of the pathogenesis, what we are certain of is that disuse and immobilization can lead to ligamentous and musculotendinous contractures as well as capsular adhesions.
Facts About Frozen Shoulder
Types of Adhesive Capsulitis:
Primary (Idiopathic) Adhesive Capsulitis: occurs spontaneously without a specific event (possibly auto-immune related).
Secondary Adhesive Capsulitis: occurs after traumatic injury, surgery, diabetes, or stroke. These cases are developed from known causes of stiffness and immobility. For the purpose of this article, we will focus on Secondary Adhesive Capsulitis as it is germane to the neurologically impaired population.
Stages of Frozen Shoulder
Reeves, in 1975, described 3 stages (painful, stiff, and recovery) of frozen shoulder:
- Freezing (Painful) Stage (2-9 months): gradual development of severe shoulder pain – worse at night with increasing stiffness. Typically, pain precedes the restriction of movement, but in some instances, loss of motion may be the first symptom.
- Frozen (Stiffness) Stage (4-12 months): severe loss of motion with decreasing pain. Joint capsule thickens and adheres itself to the humeral head.
- Thawing Stage (5-26 months): gradual return of range of motion.
Possible Causes of Frozen Shoulder
Damage to the sensory and motor areas of the cerebral cortex and brain stem leads to weakness, decreased motor control/sensation, and hyper/hypotonicity. These common clinical findings lead to limited functional movement and learned non-use. Lang et. al found that rehabilitation inpatients with hemiparesis only used their affected upper limb a mean of 3.3 hours per day. The control subjects used their dominant hand for an average of 8.7 hours per day. Bernhardht et al. examined patients less than 14 days post stroke, reported that activity of the paretic upper-limb occurred sparingly on 7% or 38 minutes of a 9-hour day. Both articles highlight the underlying concern affecting upper limb recovery; lack of movement and learned-nonuse, regardless of the cause (and muscle group/joint for that matter), may lead to soft tissue shortening and contracture.
Loss of shoulder range of motion following a neurological disease continues to be a common complication seen in the clinic. Hemiparetic patients with limited movement often develop a capsular pattern (and pain) due to progressive adaptive changes to the collagen. Capsular pattern, originally termed by Cyriax, is described as greater limitation of ER than abduction and a greater limitation of abduction than IR, in a ratio of 3:2:1.
Because many spastic hemiparetic clients with shoulder pain have limited external rotation, one logical explanation for this progressive disease may involve the spastic adductors and internal rotators and its effects on the adaptive changes to the capsule and glenohumeral joint ligaments. Shortening of the these structures often coexist with spasticity and shortening of the internal rotators (i.e., subscapularis, teres major, latissimus dorsi, pectoralis, anterior deltoid). The aforementioned shortening may lead to irritation and micro-traumatic injury to affected capsular fibers causing inflammation, pain, loss of movement, and eventually contracture and adhesions.
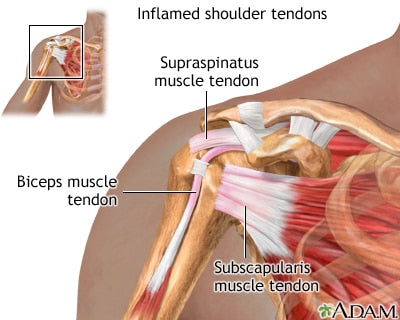
In addition to capsular restrictions from limited mobility, another possible cause of Frozen Shoulder is the spreading of an inflammatory reaction from the rotator cuff tendons and/or bursal layers to the joint capsule. Patients with Frozen Shoulder (spastic or flaccid) exhibit deficits in shoulder kinematics that can lead to subacromial inflammation (rotator cuff tendinitis/bursitis).
Scapular Dyskinesis
Spastic hemiparetic shoulder muscles resulting in altered mechanics can provoke impingement causing rotator cuff tendons to experience repetitive trauma and tissue damage. For instance, often times there is a delay in scapular upward rotation due to increased tone in scapular muscles (rhomboids, levator scapulae, and pectoralis minor) that retract/adduct, downwardly rotate and depress. This leads to subacromial trauma during faulty positioning, PROM or aggressive stretching just to name a few.
Spastic Humeral Adductors/IR’s
Often times, flexor synergy patterns present with internal rotation and adduction of the shoulder. The overactive muscles responsible for this pattern mainly include subscapularis, pectoralis major, latissimus dorsi, and teres major.
In normal circumstances, nerve impulses to the internal rotators (primarily subscapularis) are inhibited during ER and arm elevation. The muscles are deactivated allowing the humerus to externally rotate and abduct so the greater tuberosity can clear the acromion and avoid impingement when elevating the humerus. When hypertonicity is present, the subscapularis (in this example) is unable to relax, or shut off, which limits external rotation and arm elevation. This can result in impingement and subacromial inflammation leading to capsulitis.
It is important to note that impingement is not always the culprit when suffering from rotator cuff tendinitis. A prolonged shortened agonist can become painful due to constant tension. This can lead to tendinitis by itself or be the result due to painful stretching (external rotation direction). Gagliano found that spasticity-induced overload on the tendons can lead to repeated strain resulting in tissue weakness and more susceptible to damage from cumulative loading consistent with tendonopathy.
Although spasticity may play a role in the onset of Frozen Shoulder, we cannot ignore the pathomechanics of a flaccid upper limb and how it may also contribute to an inflammatory reaction. As a reminder, Frozen Shoulder can be caused by a limitation in movement or an inflammatory reaction to the joint capsule. It is similar to the “chicken or the egg” concept. Which came first? For example, in a flaccid subluxed patient who exhibits good range of motion, inflammation from a tissue injury can lead to capsulitis. During the flaccid stage, the patient typically exhibits a loss of muscle tone and voluntary movement. The humeral head stability in the glenoid fossa is diminished due to supraspinatus and deltoid weakness (proximal migrators). Gravitational forces applied to the hypotonic arm stretches the inert and non-inert structures to the point that the humeral head migrates distally below the glenoid fossa causing a subluxation.
The supraspinatus, and possibly other cuff tendons, exhibit increased tensile load because the deltoid fails to sustain the downward force of the humerus due to gravity. Prolonged tensile overload can cause mechanical fatigue, loss of elasticity and eventually inflammation and a possible tear. This inflammation can lead to adhesive capsulitis that then catapults the “Freezing Stage” described above by Reeves. Although there is conflicting evidence regarding the relationship between subluxation and pain, data does suggest that sustained elongation of inert and non-inert structures can create an inflammatory reaction that could lead to pain and further injury.
Unfortunately, when it comes to pain and stiffness, the cards are stacked against neurological patients suffering from hemiparesis. Frozen Shoulder can be a self-perpetuating process for many of our clients that fall into the moderately to severely impaired category. The faulty scapulohumeral mechanics can cause subacromial impingment that may lead to tendon damage (spreading the inflammation to the joint capsule triggering the Freezing Stage) and further atrophy. In addition, lack of use due to pain will result in capsular tightness causing, you guessed it, more impingement and inflammation.
If our clients are lucky enough to escape impingement, they may acquire rotator cuff tensile overload (if flaccid with a subluxation) or spasticty induced overload (if experiencing hypertonicity). These inflammatory conditions can also lead to pain, capsular stiffness, and future impingement. Now, not to be a “Debbie Downer”, not everyone will exhibit this debilitating condition or acquire a stiff shoulder in general. To put you in an even better mood, there are effective ways to prevent and treat Frozen Shoulder and reverse its course (I will discuss this in a future posting).
By no means are the above examples all-inclusive or comprehensive, however, it does highlight the more common causes seen in the clinic when treating hemiparetic shoulder pain. As Frozen Shoulder continues to be somewhat of a mystery, and much is still unknown, researchers are at least starting to pinpoint some of the reasons why it occurs. Regardless whether Frozen Shoulder is the result of capsular restriction or subacromial inflammation, it continues to be a serious disability that needs to be accurately understood and properly diagnosed in order for effective treatment to be administered.
Please post your comments about your experiences with Frozen Shoulder. What seems to work for you when battling this condtion? All thoughts/comments welcome.

Henry graduated from D’Youville College in Buffalo, NY in 1997 with a Masters degree in Occupational Therapy. He has worked in a variety of clinical settings including home health, acute, sub-acute, and outpatient rehab. Prior to leaving Burke Rehabilitation Hospital in New York in 2002, he worked as a clinical specialist in orthopedic medicine and manual therapy of the Upper Quadrant. After leaving Burke, Henry co-founded Saebo with the goal of creating innovative and life changing solutions for the physically impaired population. He currently holds over 15 patents with products that have helped over 30,000 clients regain function. Saebo’s name is an acronym for Henry’s grandmother “Sarah Eileen Booth”. Her entire life was dedicated to providing a hand to others in need. Saebo’s mission is to match her spirit, dedication, and desire to help others.
___________________________________________
Whether you are a caregiver, occupational therapist or even a stroke survivor yourself, Saebo provides stroke survivors young or old access to transformative and life changing products. We pride ourselves on providing affordable, easily accessible, and cutting-edge solutions to people suffering from impaired mobility and function. We have several products to help with the stroke recovery and rehabilitation process. From the SaeboFlex, which allows clients to incorporate their hand functionally in therapy or at home, to the SaeboMAS, an unweighting device used to assist the arm during daily living tasks and exercise training, we are commitment to helping create innovative products for stroke recovery. Check out all of our product offerings or let us help you find which product is right for you.
All content provided on this blog is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. If you think you may have a medical emergency, call your doctor or 911 immediately. Reliance on any information provided by the Saebo website is solely at your own risk.